
Evaluation of Gestation: Overview, Clinical Methods of Estimating Gestational Age, Estimating the Delivery Date
The introduction of obstetric ultrasonography in the early 1970s led to a marked improvement in the evaluation of fetal and placental anatomy, as well as fetal growth. Now, it is by far the most accurate technique for estimating gestational age (GA). Most pregnant women have a first trimester scan, followed by a detailed scan for anomalies in the second trimester. According to ACOG, if an ultrasound examination that confirms or revises the EDD is not performed before 22 0/7 weeks of gestational age, the pregnancy should be considered suboptimally dated.
[2]
Other documented benefits of obstetric ultrasonography include the detection of multiple pregnancies and fetal abnormalities, and the identification of placenta previa.
Ultrasonography in the first trimester
In the early first trimester, when no structures are visible within the gestational sac, GA may be estimated from the sac diameter. Several formulas can accomplish this. A common method is to measure the mean sac diameter (MSD), by calculating the mean of the 3 sac diameters. GA is then determined by consulting a table. An alternative simpler method is to add 30 to the sac size in millimeters, to give GA in days. By the time the embryo becomes visible on ultrasound the sac diameter is no longer accurate in estimating gestational age.
If cardiac activity can be detected but the embryo is not measurable, the GA is about 5.5-6.0 weeks.
GA in the first trimester is usually calculated from the fetal crown-rump length (CRL). This is the longest demonstrable length of the embryo or fetus, excluding the limbs and the yolk sac.

Ultrasonographic view of a fetus for a crown-rump measurement.
View Media Gallery
The correlation between CRL and GA is excellent until approximately 12 weeks’ amenorrhea. No sex or race differences are appreciable, but maternal characteristics, such as age and smoking, may have a significant effect beyond 10 week’ gestation. The GA estimate has a 95% confidence interval of plus or minus 6 days, and it is most accurate between 7 and 10 weeks’ amenorrhea. The following formula
[7] allows the estimation of GA (weeks) from the CRL (mm):
GA = –0.0007 (CRL)2 + 0.1584 (CRL) + 5.2876
Transabdominal ultrasonography may underestimate gestational age by an average of 1.6 days compared with transvaginal ultrasonography.
[8]
In twin pregnancies, the CRL of the smaller fetus is more accurate in determining gestational age.
[9]
The biparietal diameter measured between 9 and 13 weeks’ gestation has recently been shown to be at least as accurate as the CRL,
[10] with smaller random errors.
A study by Skupski et al developed a new formula to estimate gestational age from biometric data on ultrasound. The new formula was: GA = 7.85-0.127 * biparietal diameter + 0.07304 * head circumference + 0.00638 * abdominal circumference + 0.122 * femur length + 0.000685 * biparietal diameter * abdominal circumference – 0.00015 * head circumference * abdominal circumference.
[11, 12]
Ultrasonography in the second trimester
Fetal biometry in the second trimester can yield acceptably accurate estimates of GA from 12 to approximately 22 weeks of amenorrhea.
[7] Recent work has shown that the accuracy of ultrasonographic biometry at 12-14 weeks’ gestation is at least as good as biometry performed after 14 weeks.
[13, 14] The best parameters are the biparietal diameter (BPD) and the head circumference (HC), which are virtually linearly related to GA.

Ultrasonographic image of a fetal head, with measurement of the head circumference.
View Media Gallery
The femur length (FL) can also be used and is nearly as accurate as head measurements.
[15]
Ultrasonographic view of a fetal femur.
View Media Gallery
Racial differences in FL are significant, but differences in HC are not. GA estimates by the BPD or HC have a 95% confidence interval of plus or minus 8 days. The following formula
[16] allows estimation of GA (days) from the BPD (mm):
GA = 39.1 + 2.1 (BPD)
Combinations of multiple variables to date a pregnancy have also been described; however, the improvement in accuracy from these algorithms is clinically negligible.
Ultrasonography in the third trimester
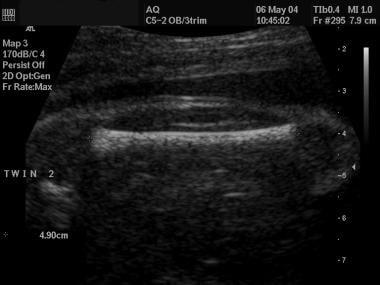
Fetal biometry in the third trimester is subject to much greater individual size variations than in the second trimester. Its accuracy for GA assignment is reduced considerably, and estimates may have confidence intervals of plus or minus 3 weeks.
[17] More recent work with pregnancies resulting from in vitro fertilization suggests that third trimester scans are considerably more accurate than previously thought, with random errors (1 SD) of 8-9 days. This is equivalent to confidence intervals of about plus or minus 2 weeks.
[18]
The table below illustrates the 95% confidence limits for GA estimated from the BPD in the third trimester.
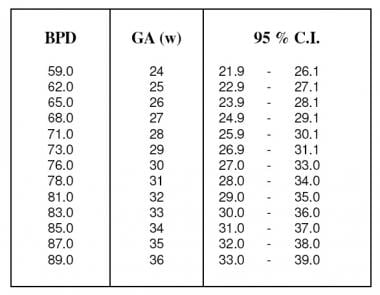
Estimate of gestational age (weeks) from the biparietal diameter in the third trimester with 95% confidence intervals. Adapted from Hadlock et al (1984).
View Media Gallery
Confirmation of fetal maturity may also be obtained by examining the ossification centers.
[19] The distal femoral epiphysis appears at a mean age of 32-33 weeks’ gestation, but may be seen as early as 29 weeks’ gestation
[20] ; its size increases linearly with gestational age. A distal femoral epiphysis diameter greater than 7 mm indicates a gestational age greater than 37 weeks. Visualization of the proximal tibial epiphysis indicates a gestational age of at least 35 weeks. The sonographic detection of the proximal humeral epiphysis has been correlated with a mature amniocentesis lung profile.





